
Abstract
Millions of people die every year from diseases caused by exposure to outdoor air pollution1,2,3,4,5. Some studies have estimated premature mortality related to local sources of air pollution6,7, but local air quality can also be affected by atmospheric transport of pollution from distant sources8,9,10,11,12,13,14,15,16,17,18. International trade is contributing to the globalization of emission and pollution as a result of the production of goods (and their associated emissions) in one region for consumption in another region14,19,20,21,22. The effects of international trade on air pollutant emissions23, air quality14 and health24 have been investigated regionally, but a combined, global assessment of the health impacts related to international trade and the transport of atmospheric air pollution is lacking. Here we combine four global models to estimate premature mortality caused by fine particulate matter (PM2.5) pollution as a result of atmospheric transport and the production and consumption of goods and services in different world regions. We find that, of the 3.45 million premature deaths related to PM2.5 pollution in 2007 worldwide, about 12 per cent (411,100 deaths) were related to air pollutants emitted in a region of the world other than that in which the death occurred, and about 22 per cent (762,400 deaths) were associated with goods and services produced in one region for consumption in another. For example, PM2.5 pollution produced in China in 2007 is linked to more than 64,800 premature deaths in regions other than China, including more than 3,100 premature deaths in western Europe and the USA; on the other hand, consumption in western Europe and the USA is linked to more than 108,600 premature deaths in China. Our results reveal that the transboundary health impacts of PM2.5 pollution associated with international trade are greater than those associated with long-distance atmospheric pollutant transport.
Similar content being viewed by others

Main
Outdoor air pollution and the associated effects on health have typically been regarded as local or regional problems, with local or regional solutions. In response to the health risk caused by exposure to outdoor air pollution, many countries have adopted environmental policies to regulate major sources of outdoor air pollution such as industry, agriculture and transportation within their territories25. However, it is also increasingly recognized that air quality in a given location can be substantially affected by atmospheric transport of pollution from distant sources, including sources on other continents8,9,10,11,12,13,14. This transport of pollution indicates that premature mortality related to air pollution (that is, death of an individual before his or her life expectancy due to exposure to air pollution) is not only a local issue12,15,16,17,18. International trade is further globalizing the issue of air-pollution-related mortality by separating the locations where goods are consumed from the locations where the emissions and related pollution and mortality occur. Here we combine four state-of-the-art global models to estimate the premature mortality linked to global PM2.5 (fine particulate matter with an aerodynamic diameter of 2.5 μm or less) air pollution; we attribute the global premature deaths not only to the pollution physically produced within the different regions, but also to pollution related to goods and services that are ultimately consumed in each region. We estimate premature mortality resulting from only PM2.5 pollution because previous studies have shown that this type of pollution accounts for more than 90% of the global mortality from outdoor air pollution1,5.
Beginning with a newly developed emissions inventory of primary air pollutants produced in 13 world regions in 2007 (Extended Data Fig. 1), we use a multi-regional input–output model of international trade to identify and isolate the emissions related to consumption and investment in each region in that year. (The methodology and data used for developing the production- and consumption-related emissions inventory is provided in Supplementary Information.) We then track the globally distributed PM2.5 pollution that is contributed by emissions produced in each region and by emissions associated with consumption in each region using the chemical transport model GEOS-Chem26. Next, following the methods of the Global Burden of Disease (GBD) Study1, we estimate the premature mortality due to exposure to outdoor PM2.5 related to production and consumption in each region; we apply the GEOS-Chem-modelled regional fractional contributions to mortality calculated using the high-resolution PM2.5 concentrations from the GDB Study of 201327. PM2.5-related premature mortality linked to ischaemic heart disease, stroke, lung cancer and chronic obstructive pulmonary disease is calculated by using an integrated exposure model2 that estimates the risk of premature mortality from each of the four diseases at different levels of exposure to PM2.5. Because errors propagated across multiple global models can be large, we conducted uncertainty analyses and made comparisons with independent data12,13,18,27,28 to demonstrate the robustness of our main findings. A description of these models, their integration and uncertainty, comparisons with other studies, and a comprehensive listing of all data sources and key references are provided in Methods and Supplementary Information.
We estimate that PM2.5-related premature mortality in 2007 was 3.45 million (95% confidence interval (CI), 2.38–4.14 million; Extended Data Table 1; compare with 3.22 million deaths in 2010 reported by the GBD Study1 and 3.15 million in 2010 by Lelieveld et al.6). Of this total, we attribute 2.52 million deaths (73.0%; 95% CI, 1.74–3.02 million deaths) to production activities in specific regions. The related production sectors include energy, industry, transportation, residential (both fossil fuels and biofuels) and agriculture. The remaining deaths are related to emissions from international shipping and aviation, which are difficult to assign to specific regions, or to emissions from natural sources such as biogenic emissions, field burning, forest fires and mineral dust, which are not directly related to consumption. Unless stated otherwise, the numbers of premature deaths reported hereafter correspond to only the deaths attributable to emissions from an identifiable production sector in a specific region (‘attributable deaths’) and do not include those related to the aforementioned unassignable or non-consumption-related emissions, and reflect median estimates rounded to the nearest hundred.
Figure 1a–d shows the global spatial distribution of premature deaths in 2007 due to PM2.5 air pollution produced in China, western Europe, the USA and India, respectively (see Extended Data Fig. 2a–i for maps for other regions). In each case, the greatest health impacts of pollution produced in a given region are local, but deaths in neighbouring and more distant regions are also evident, owing to intercontinental transport, particularly in downwind areas with dense populations. Our results are broadly consistent with previous transboundary pollution studies12,13,18, given the differences in methodology (Supplementary Information).

a–h, Maps show the number of deaths related to either the air pollution produced (that is, emitted) in the given region (a, China; b, western Europe; c, USA; d, India) or the air pollution related to goods and services consumed in that region (e–h). Differences in worldwide premature mortality between production- and consumption-related PM2.5 air pollution for these four regions are presented in Extended Data Fig. 4.
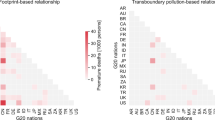
Figure 2a shows the percentage of deaths in each region due to emissions in that and other regions. As expected, hotspots of mortality due to transboundary pollution occur in populous neighbouring regions. For example, 30,900 (95% CI, 14,100–47,700) deaths in the ‘rest of east Asia’ region (which includes Japan and South Korea) were related to emissions in China (Figs 1a, 2a) and 47,300 (95% CI, 20,300–74,400) deaths in eastern Europe were related to emissions in western Europe (Figs 1c, 2a). More distant effects are also evident: for example, 2,300 (95% CI, 1,000–3,600) deaths in western Europe were related to pollution transported from the USA. Globally, 16.3% (95% CI, 13.3%–19.3%) of the attributable deaths, or 12.0% (95% CI, 9.8%–14.2%) of total PM2.5-related deaths, were caused by pollution produced in a region other than that in which the death occurred.

Each cell in the grid shows the fraction of deaths (%) that occurred in the region indicated by the column due to pollution produced (a) or due to goods and services consumed (b) in the region indicated by the row. The diagonal thus reflects deaths in a region due to pollution produced (a) or goods and services consumed (b) in that same region. Darker shading in the off-diagonal cells highlights higher fractions. In each case, the number of attributable deaths that occurred in each region is shown at the top, and the number of worldwide deaths caused directly by pollution produced in each region (a) or indirectly by consumption of products in each region that are produced in that region or elsewhere (b) is shown at the right. Uncertainty ranges for the numbers given here are presented in Extended Data Fig. 5. The regions are defined in Extended Data Fig. 1.
In addition to the physical transport of pollution in the atmosphere, international trade has an influence on the regions where health impacts are greatest by allowing the production of emissions to occur far from where goods and services are ultimately consumed. Figure 1e–h shows the distribution of deaths in 2007 due to PM2.5 pollution related to goods and services consumed in the representative regions (see Extended Data Fig. 3a–i for maps for other regions). For each region, compared to the distribution of deaths attributable to the direct production of emissions, consumption-related deaths are scattered more widely around the world owing to international trade (Fig. 1).
Figure 2b shows the percentage of deaths in each region due to emissions related to consumption in that and other regions. Regionally, the share of deaths in a given region that are related to goods and services consumed elsewhere varies from 15.2% (95% CI, 14.2%–16.3%) in the more-isolated, less-developed region of sub-Saharan Africa to 53.7% (95% CI, 44.2%–63.2%) in the high-energy-exporting region of Russia (Fig. 2b). The transboundary health impacts related to international trade are much greater than those related to atmospheric transport. For example, 4.1% (95% CI, 1.1%–7.1%) of the attributable deaths in the USA are related to consumption in western Europe, whereas only 0.2% (95% CI, 0.1%–0.4%) are related to transboundary transport of pollution from western Europe. The ‘spillover’ effect in neighbouring regions is also noteworthy: 34.3% (95% CI, 19.9%–48.7%) of deaths in the ‘rest of east Asia’ region are attributable to the combined effects of the advection of pollution and international trade from China. Globally, 30.2% (95% CI, 25.4%–35.0%) of the attributable deaths, or 22.2% (95% CI, 18.7%–25.7%) of total PM2.5-related deaths, were caused by pollution produced in a region other than that in which the related goods and services were ultimately consumed.
International trade allows production and consumption activities to be physically separated, with emissions occurring within the region where the goods are produced and related health impacts concentrated within that producing region and nearby downwind regions, all of which might be far from the regions where those goods are ultimately consumed. Figure 3 shows the net effect of international trade on emissions, PM2.5 exposure and mortality in each region, quantified, for each parameter, as the difference between its value when assigned according to the region where goods and services were consumed and when assigned according to the location of production. Taking SO2 (a key precursor of secondary PM2.5) as an example, Fig. 3a shows the difference between where SO2 emissions were physically produced and where the related goods and services were consumed, thereby highlighting the emissions embodied in the net trade of goods and services among the 13 regions, in 2007. The most developed regions of the world, such as the USA, western Europe and the ‘rest of east Asia’ region, are importers of net embodied emissions: they tend to import goods and services from China and less-developed neighbouring areas, thereby causing pollution in those regions. China is the world’s largest exporter of embodied emissions, with large quantities of SO2 embodied in exports to the aforementioned three regions.

a–c, Maps show differences between production- and consumption-based accounting of SO2 emissions (a; in units of megatonnes of SO2 per year), population-weighted average PM2.5 exposure (b; in units of micrograms of PM2.5 per cubic metre) or premature mortality due to PM2.5 air pollution (c; deaths per year). In each case, net importers are shown in shades of red and net exporters in shades of blue. Although the emissions embodied in exports from regions such as Latin America, Canada, sub-Saharan Africa and Australia are greater than the emissions embodied in their imports (blue shading in a), the PM2.5 exposure and mortality embodied in imports to those regions are greater than the exposure and mortality embodied in their exports (red shading in b and c). The differences are due to differences in population density (b) and the marginal health impacts of emissions (c) in regions such as China, Europe, India and the ‘rest of Asia’ region (that is, central and southeast Asia), which are the source of many of the goods imported by other regions. The USA, western Europe and the ‘rest of east Asia’ region (including South Korea and Japan) are net importers of pollution, exposure and deaths. Note that Mongolia, North Korea, South Korea and Japan are grouped into a single region (‘rest of east Asia’), which tends to overemphasize the effect of trade, in Mongolia in particular.
In turn, emissions displaced via trade are transported in the atmosphere, which then affects population exposure to the pollution. Figure 3b shows the difference between global, population-weighted mean concentrations of PM2.5 due to the emissions produced in each region and those due to the emissions related to the goods and services consumed in each region—that is, the PM2.5 exposure that is embodied in net trade. Although similar to the pattern of the emissions embodied in trade (Fig. 3a), these changes in air quality highlight cases for which there are populous areas downwind of where the emissions are produced. For example, emissions embodied in Chinese exports have a disproportionately large effect on exposure in population-dense regions (for example, Japan and South Korea) that are near to and downwind of China (Figs 1, 3b).
Finally, Fig. 3c shows the PM2.5-related premature mortality embodied in net trade, which incorporates the emissions displaced via trade, the subsequent changes in air quality as pollution is transported in the atmosphere, and the health impacts of poor air quality. Given China’s population density, high emission intensity, large proportion of exports, and the large populations of neighbouring regions, Chinese exports embody a greater number of deaths than do exports from any other region (Fig. 3c). By contrast, net imports to the USA and western Europe embody the greatest number of deaths (Fig. 3c).
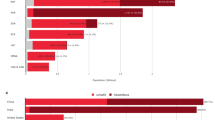
Figure 4 summarizes premature mortality due to both advection of PM2.5 air pollution and displacement of pollution via international trade with a series of bar charts. The per-capita mortality is presented in Extended Data Fig. 6 as an indicator of the emissions produced per person in a country and the relative health impacts of those emissions (see details in Methods). Figure 4a shows that emissions produced in China cause more than twice the number of deaths worldwide than do the emissions produced in any other region, followed by emissions produced in India and the ‘rest of Asia’ region. Figure 4e shows that when these deaths are allocated according to where the related goods and services are consumed, China and India still dominate, consistent with the health impacts of air pollution being mostly local; however, the roles of western Europe and the USA are also highlighted by the consumption-based perspective (Fig. 4a, e).

a, e, Worldwide mortality due to pollution produced (that is, emitted) in each region (a) or related to products consumed in each region (e). b, f, Mortality in each region due to pollution produced in that region (b) or related to products consumed in that region (f). c, g, Mortality in all other regions due to pollution produced in each region (c) or related to products consumed in each region (g). Note that the number of deaths in each region in b and c (f and g) therefore sum to those in the same region in a (e). d, h, Mortality in each region due to pollution produced elsewhere (d) or related to products consumed elsewhere (h). The numbers down the left-hand side of each panel give the number of deaths in 2007 (in units of 105). Error bars denote 95% CIs, determined by uncertainties in the GEOS-Chem-simulated fractional contribution of PM2.5 exposure and in the total PM2.5-related mortality.
Figure 4d shows the premature mortality in each region due to emissions produced in other regions, revealing the substantial health impacts of transboundary pollution in the ‘rest of east Asia’ region, India and eastern Europe. When trade effects are also included, the transboundary health impacts increase markedly, particularly in China and other emerging markets (for example, India and Russia), and in more-developed downwind regions (for example, the ‘rest of east Asia’ region, which includes Japan and South Korea) (Fig. 4h). In turn, consumption in western Europe, the USA and the ‘rest of Asia’ region corresponds to the greatest number of deaths in other regions (Fig. 4g).
Our findings quantify the extent to which air pollution is a global problem. In our global economy, the goods and services consumed in one region may entail production of large quantities of air pollution—and related mortality—in other regions. If the cost of imported products is lower because of less stringent air pollution controls in the regions where they are produced, then the consumer savings may come at the expense of lives lost elsewhere29,30. Regional policies that regulate air quality by imposing a price on pollutant emissions may be effective, and in some cases a considerable proportion of the overall costs of such policies might be shared with consumers in other regions (see Fig. 3a). However, there is some evidence that the polluting industries have tended to migrate to regions with more permissive environmental regulations29,30, suggesting that there may be tension between efforts to improve air quality in a given region and to attract direct foreign investment. Improving pollution control technologies in China, India and elsewhere in Asia would have a disproportionately large health benefit in those regions and worldwide, and international cooperation to support such pollution abatement efforts and to reduce ‘leakage’ of emission via international trade is in the global interest.
Methods
Integrated model framework
This study required integration of data, models and methods from multiple sources and scientific disciplines, as depicted in Extended Data Fig. 7. We first developed a global inventory of all major sources of anthropogenic air pollution emissions in 228 countries and regions for the year 2007, disaggregating emissions from 62 subsectors (as opposed to aggregated sectors in available global inventories). We then used a global multi-regional input–output model (MRIO)31,32 based on data from the Global Trade Analysis Project (GTAP)33 to re-attribute the emissions produced by these different sectors according to the demand of consumers for finished goods. The MRIO thus traces all emissions related to consumed goods back to the original sources of produced emissions, even if the supply chain of the consumed products encompasses intermediate inputs (for example, parts) and services (for example, assembly and transport) from multiple sectors across multiple regions. Prior to the re-attribution, the production-based global emission inventory was mapped to 129 regions and 57 sectors in GTAP to facilitate the MRIO analysis. Next, we used the GEOS-Chem chemical transport model26 to track physical transport of emissions in the atmosphere, obtaining the fractional contribution of each region to global near-surface PM2.5 concentrations from both production and consumption perspectives by a zero-out approach. These derived ratios were multiplied by high-resolution global PM2.5 concentration data27 developed for the Global Burden of Disease Study of 2013 (GBD2013) to obtain the PM2.5 exposure levels from both production and consumption perspectives. Given the computational constraints of the chemical transport model, the GEOS-Chem modelling required further geographical aggregation. We classified the world into 13 regions on the basis of their level of economic development, regions in the trade model and levels of air pollution: China, rest of east Asia, India, rest of Asia, Russia, western Europe, eastern Europe, Middle East and north Africa, USA, Canada, Latin America, sub-Saharan Africa and rest of the world. The classifications used to sort the 228 countries into these 13 regions are shown in Supplementary Table 1 and Extended Data Fig. 1. Finally, we applied the Integrated Exposure-Response (IER) model2 to evaluate the effect of changes in PM2.5 concentrations to premature mortality, summing across regions to obtain the global PM2.5 mortality related to both emissions produced and goods consumed in each region. See Supplementary Information for further details of all of the above steps.
We conducted comprehensive uncertainty analyses, integrating errors in all steps, and compared our results with independent data. In summary, we estimate uncertainty (P = 0.005) associated with production-based emissions using distributions of key parameters derived from the literature, expert judgments and measurement data for each industrial subsector in each of the 13 regions. Our estimates are generally consistent with the HTAP v2.2 emission inventory28, which represents the state-of-the-art understanding of global emissions. We also evaluated uncertainty related to our modelling of atmospheric transport (including sensitivity analyses of nonlinear effects and neglected emissions of non-methane volatile organic compounds) and compared our results to both ground-based observations and GBD PM2.5 concentrations. Our results on transboundary transport of PM2.5 are generally consistent with the HTAP study13 when harmonizing the model domain and target species. We assessed the uncertainties of our mortality estimates by varying the applicable parameters in our IER model across 1,000 trials; our estimates of mortality are very close to those from the GBD Study1 and by Lelieveld et al.6. Details of these analyses are presented in Supplementary Information.
Per-capita mortality due to transported pollution and traded products
Extended Data Fig. 6a shows that the emissions produced per one million people in eastern Europe result in 1,027 (95% CI, 749–1,306) PM2.5-related deaths around the world—a greater impact per capita than any other region. Having the world’s largest population, per-capita impacts in China are quite substantial: the emissions produced per one million people in China cause 770 (95% CI, 529–1,014) deaths worldwide (Extended Data Fig. 6a). In terms of consumption, consumers in affluent regions such as western Europe, the USA and Canada are associated with a greater-than-average number of PM2.5-related deaths worldwide (Extended Data Fig. 6e). Further, a disproportionate number of those deaths occurred in regions other than that in which the products were consumed: for every one million consumers in western Europe, Canada and the USA, 416 (95% CI, 303–530), 395 (95% CI, 268–522) and 339 (95% CI, 231–448) PM2.5-related deaths, respectively, occurred in other regions (Extended Data Fig. 6g). Per capita, eastern Europe and Russia suffered more of these transboundary deaths than did any other region: per one million people in those regions, 531 (95% CI, 335–727) and 365 (95% CI, 278–453) died, respectively, as a result of products consumed elsewhere (Extended Data Fig. 6h).
Data availability
The datasets generated during this study are available from the corresponding author on reasonable request. Source Data for Figs 2, 3, 4 and Extended Data Figs 5 and 6 are available in the online version of the paper.
References
Lim, S. S. et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380, 2224–2260 (2012)
Burnett, R. T. et al. An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ. Health Perspect. 122, 397–403 (2014)
Pope, C. A. et al. Lung cancer, cardiopulmonary mortality and long-term exposure to fine particles air pollution. J. Am. Med. Assoc. 287, 1132–1141 (2002)
Cohen, A. J. et al. The global burden of disease due to outdoor air pollution. J. Toxicol. Environ. Health A 68, 1301–1307 (2005)
Forouzanfar, M. H. et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 386, 2287–2323 (2015)
Lelieveld, J., Evans, J. S., Fnais, M., Giannadaki, D. & Pozzer, A. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 525, 367–371 (2015)
Chafe, Z. A. et al. Household cooking with solid fuels contributes to ambient PM2.5 air pollution and the burden of disease. Environ. Health Perspect. 122, 1314–1320 (2014)
Akimoto, H. Global air quality and pollution. Science 302, 1716–1719 (2003)
Jaffe, D. et al. Transport of Asian air pollution to North America. Geophys. Res. Lett. 26, 711–714 (1999)
Cooper, O. R. et al. A case study of transpacific warm conveyor belt transport: influence of merging airstreams on trace gas import to North America. J. Geophys. Res. 109, D23S08 (2004)
Verstraeten, W. W. et al. Rapid increases in tropospheric ozone production and export from China. Nat. Geosci. 8, 690–695 (2015)
Liu, J., Mauzerall, D. L. & Horowitz, L. W. Evaluating inter-continental transport of fine aerosols: (2) global health impact. Atmos. Environ. 43, 4339–4347 (2009)
Dentener, F., Keating, T. & Akimoto, H. (eds) Hemispheric Transport of Air Pollution 2010. Part A: Ozone and Particulate Matter. Report No. ECE/EN.AIR/100, Air Pollution Studies No. 17, 135–215 (UNECE, 2010)
Lin, J. et al. China’s international trade and air pollution in the United States. Proc. Natl Acad. Sci. 111, 1736–1741 (2014)
Duncan, B. N., West, J. J., Yoshida, Y., Fiore, A. M. & Ziemke, J. R. The influence of European pollution on ozone in the Near East and northern Africa. Atmos. Chem. Phys. 8, 2267–2283 (2008)
West, J. J., Naik, V., Horowitz, L. W. & Fiore, A. M. Effect of regional precursor emission controls on long-range ozone transport – part 2: steady-state changes in ozone air quality and impacts on human mortality. Atmos. Chem. Phys. 9, 6095–6107 (2009)
Anenberg, S. C. et al. Intercontinental impacts of ozone pollution on human mortality. Environ. Sci. Technol. 43, 6482–6487 (2009)
Anenberg, S. C. et al. Impacts of intercontinental transport of anthropogenic fine particulate matter on human mortality. Air Qual. Atmos. Health 7, 369–379 (2014)
Davis, S. J. & Caldeira, K. Consumption-based accounting of CO2 emissions. Proc. Natl Acad. Sci. 107, 5687–5692 (2010)
Peters, G. P., Minx, J. C., Weber, C. L. & Edenhofer, O. Growth in emission transfers via international trade from 1990 to 2008. Proc. Natl Acad. Sci. 108, 8903–8908 (2011)
Liu, J. et al. Systems integration for global sustainability. Science 347, 1258832 (2015)
Oita, A. et al. Substantial nitrogen pollution embedded in international trade. Nat. Geosci. 9, 111–115 (2016)
Zhao, H. et al. Assessment of China’s virtual air pollution transport embodied in trade by a consumption-based emission inventory. Atmos. Chem. Phys. 15, 5443–5456 (2015)
Jiang, X. et al. Revealing the hidden health costs embodied in Chinese exports. Environ. Sci. Technol. 49, 4381–4388 (2015)
Zhang, Q., He, K. & Huo, H. Policy: cleaning China’s air. Nature 484, 161–162 (2012)
Bey, I. et al. Global modeling of tropospheric chemistry with assimilated meteorology: model description and evaluation. J. Geophys. Res. 106, 23073–23095 (2001)
Brauer, M. et al. Ambient air pollution exposure estimation for the global burden of disease 2013. Environ. Sci. Technol. 50, 79–88 (2016)
Janssens-Maenhout, G. et al. HTAP_v2.2: a mosaic of regional and global emission grid maps for 2008 and 2010 to study hemispheric transport of air pollution. Atmos. Chem. Phys. 15, 11411–11432 (2015)
Levinson, A. & Taylor, M. S. Unmasking the pollution haven effect. Int. Econ. Rev. 49, 223–254 (2008)
Kanemoto, K., Moran, D., Lenzen, M. & Geschke, A. International trade undermines national emission reduction targets: new evidence from air pollution. Glob. Environ. Change 24, 52–59 (2014)
Peters, G. P., Andrew, R. & Lennox, J. Constructing an environmentally-extended multi-regional input-output table using the GTAP database. Econ. Syst. Res. 23, 131–152 (2011)
Andrew, R. M. & Peters, G. P. A multi-region input-output table based on the global trade analysis project database (GTAP-MRIO). Econ. Syst. Res. 25, 99–121 (2013)
Badri, N., Angel, A. & Robert, M. (eds) Global Trade, Assistance, and Production: The GTAP 8 Data Base (Center for Global Trade Analysis, Purdue University, 2012)
Acknowledgements
This work is supported by the National Natural Science Foundation of China (41625020, 41629501, 41422502, 41222036 and 41541039) and China’s National Basic Research Program (2014CB441301 and 2014CB441303). Q.Z. and K.H. are supported by the Collaborative Innovation Center for Regional Environmental Quality and the Cyrus Tang Foundation. The work at Argonne National Laboratory acknowledges the Modeling, Analysis and Predictability (MAP) programme of the National Aeronautics and Space Administration (NASA) under Proposal No. 08-MAP-0143, for which we thank D. Considine (NASA) and M. Chin (NASA Goddard Space Flight Center). H.H. acknowledges the support of the National Natural Science Foundation of China (71322304). Z.L. acknowledges the support from the National Natural Science Foundation of China (41501605). D.G. acknowledges the support from the National Key R&D Program of China (2016YFA0602604), the UK Economic and Social Research Council (ES/L016028/1), the UK Natural Environment Research Council (NE/N00714X/1), and the British Academy (AF150310). We thank T. Xue for discussions on statistics.
Author information
Authors and Affiliations
Contributions
Q.Z., J.L. and K.H. conceived the study. Q.Z. led the study. Z.Lu and D.G.S. provided emissions data. M.B., A.v.D. and R.V.M. provided PM2.5 exposure data. D.T., H.Z., T.F. and D.G. calculated emissions. G.G. conducted GEOS-Chem simulations. X.J. conducted estimates of health impacts. Q.Z., X.J., S.J.D., G.G. and J.L. interpreted the data. Q.Z., X.J., D.T., S.J.D., H.Z. and G.G. wrote the paper with input from all co-authors.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Additional information
Reviewer Information Nature thanks G. Janssens-Maenhout, P. Jha and the other anonymous reviewer(s) for their contribution to the peer review of this work.
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data figures and tables
Extended Data Figure 2 Global distribution of premature mortality in 2007 due to production-related PM2.5 air pollution.
a–i, Maps show the number of deaths related to air pollution produced (that is, emitted) in the rest of east Asia (a), the rest of Asia (b), Russia (c), eastern Europe (d), Canada (e), the Middle East and north Africa (f), Latin America (g), sub-Saharan Africa (h) and the rest of the world (i).
Extended Data Figure 3 Global distribution of premature mortality in 2007 due to consumption-related PM2.5 air pollution.
a–i, Maps show the number of deaths related to goods and services consumed in the rest of east Asia (a), the rest of Asia (b), Russia (c), eastern Europe (d), Canada (e), the Middle East and north Africa (f), Latin America (g), sub-Saharan Africa (h) and the rest of the world (i).
Extended Data Figure 4 Differences in worldwide premature mortality in 2007 between production- and consumption-related PM2.5 air pollution.
a–d, Maps show the number of deaths worldwide related to consumption in the given region minus the number of deaths worldwide related to production in that region, for China (a), western Europe (b), the USA (c) and India (d).
Extended Data Figure 5 Uncertainty ranges.
a, b, Uncertainties relating to Fig. 2. The ranges at the top of each panel represent the 95% CI for the number of attributable deaths in the region indicated by the column. The ranges at the right of each panel represent the 95% CI for the total number of worldwide deaths caused by pollution produced in the region indicated by the row (a) or related to the consumption of products in that region that are produced there or elsewhere (b). Each cell in the grid shows the standard deviation of the fraction of deaths (%); darker shading in the off-diagonal cells highlights larger standard deviations.
Extended Data Figure 6 Summary of global premature mortality per capita due to transported PM2.5 pollution and traded products.
a, e, Worldwide mortality due to pollution produced (that is, emitted) in each region (a) or related to products consumed in each region (e). b, f, Mortality in each region due to pollution produced in that region (b) or related to products consumed in that region (f). c, g, Mortality in all other regions due to pollution produced in each region (c) or related to products consumed in each region (g). d, h, Mortality in each region due to pollution produced elsewhere (d) or related to products consumed elsewhere (h). All data are normalized according to regional populations (reported as deaths per one million people). Error bars denote 95% CIs, determined by uncertainties in the GEOS-Chem-simulated fractional contribution of PM2.5 exposure and in the total PM2.5-related mortality.
Supplementary information
Supplementary Information
This file contains Supplementary Text and Data, additional references, Supplementary Figures 1-10, Supplementary Tables 5, 7 and 8 (see separate excel files for Supplementary Tables 1-4 and 6). (PDF 3234 kb)
Supplementary Table 1
This file contains country lists in the alternate emission inventory and the GTAP model, and the corresponding classification of 13 regions. (XLSX 18 kb)
Supplementary Table 2
This file contains the sources category of the emission inventory in this study. (XLSX 14 kb)
Supplementary Table 3
This file contains mapping structure from emission inventory to GTAP sectors. (XLSX 22 kb)
Supplementary Table 4
This file contains mapping structure from EDGAR sectors to GTAP sectors. (XLSX 13 kb)
Supplementary Table 6
This file contains camparison of transboundary transport of PM2.5 with the HTAP study. (XLSX 12 kb)
Rights and permissions
About this article

Cite this article
Zhang, Q., Jiang, X., Tong, D. et al. Transboundary health impacts of transported global air pollution and international trade. Nature 543, 705–709 (2017). https://doi.org/10.1038/nature21712
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nature21712
This article is cited by
-
Inequality in economic shock exposures across the global firm-level supply network
Nature Communications (2024)
-
Global transboundary synergies and trade-offs among Sustainable Development Goals from an integrated sustainability perspective
Nature Communications (2024)
-
Seasonal variation, source apportionment, and cancer risk assessment of PM2.5-bound phthalates: a case study in Taiyuan, China
Air Quality, Atmosphere & Health (2024)
-
Contribution of local and surrounding anthropogenic emissions to a particulate matter pollution episode in Zhengzhou, Henan, China
Scientific Reports (2023)
-
Ecologically unequal exchanges driven by EU consumption
Nature Sustainability (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
